But to keep this short...
Cordain contends:
"There are components in raw cereal grains which wreak absolute havoc with human health and well-being." ... Besides phytates, "these antinutrients include protease inhibitors, alkylrescorcinols, alpha-amylase inhibitors, molecular-mimicking proteins, etc."He adds that sophisticated processing technologies only partially mitigate the negative effect of grain consumption.
He lays out a convincing argument.
I have 2 concerns. When we choose not to eat grains, legumes, starchy tubers, and dairy foods, we're left with meat, seafood, fruit, vegetables, nuts, and a few other seeds - all foods promoted in the Paleo Diet.
Concern 1. Virtually ALL plant foods contain some amount of toxin or antinutrient, not just grains (which are seeds of grasses), legumes, and potatoes. Below is a table I swiped from Cornell University's GEO-PIE site.1
If we are to apply the antinutrient argument to the selection of our meals, why not limit consumption of all plant foods? That leads me to my next concern.
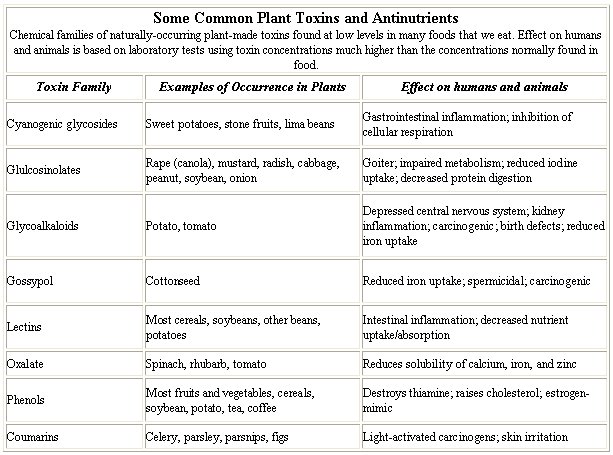
Concern 2. Animal tissue is also a source of toxins. Just as mercury bioaccumulates in fish (fish higher up the food chain contain more mercury), so chemicals, some toxic, can bioaccumulate in an ecosystem. Below is some text that accompanied the above table:
"Many of these compounds are known carcinogens. Some fat-soluble plant toxins even bioaccumulate - that is, when an animal eats the plant, the toxins collect in animal tissues and pass to humans when we eat the animal - and can be secreted in human and animal milk (for example, solanine from potatoes)."
 And if it's grain we're trying to avoid, let us not look to our livestock, whose cells are packed with the imprint of the grain used to fatten them. In The Omnivore's Dilemma,
And if it's grain we're trying to avoid, let us not look to our livestock, whose cells are packed with the imprint of the grain used to fatten them. In The Omnivore's Dilemma,"The higher the ratio of carbon 13 to carbon 12 in a person's flesh, the more corn has been in his diet - or in the diet of the animals he or she ate."In fact, he says, when you compare the tissues of Mexicans, who eat more corn (outright) than North Americans, you find they still have a lower concentration of corn-based carbon 13 isotope in their bodies than we do. Our corn-fed cattle, and our consumption of same, are contributing to claims such as Todd Dawson, a Berkeley biologist made in reference to our corny tissues, "North Americans look like corn chips with legs."
Given the plethora of harmful compounds that Cordain describes reside in cereal grains, I shiver to think what amount of them may be accumulating in the flesh of our grain-fed livestock.
If we are to apply the antinutrient argument to the selection of our meals, why not limit consumption of animal foods as well as plant foods? (Let this be one more argument for pastured livestock.)
The Paleo Diet shows the potential of being the mother of all weight loss diets.
2 Charming photograph of snake/frog/insect food chain via Biomes Blog.


 The Sunday New York Times Magazine runs a feature called Diagnosis. The November 12th issue described a man who presented with a wound (an incision from a hernia operation) that would not heal ("
The Sunday New York Times Magazine runs a feature called Diagnosis. The November 12th issue described a man who presented with a wound (an incision from a hernia operation) that would not heal ("

 Does policosanol lower cholesterol or doesn't it?
Does policosanol lower cholesterol or doesn't it?

 There seems to be a holdup on marketing of GlaxoSmithKline's (GSK) new over-the-counter (OTC) weight-loss drug, Alli. In an 11 to 3 vote, an FDA advisory panel recommended approval of Alli, the OTC version of Xenical, on January 23 - over 9 months ago. GSK was thrilled and hoped to get the drug in stores before the end of this year, pending the FDA's final go-ahead. Since Alli would be the only FDA-approved weight-loss drug available without a prescription, GSK was salivating.
There seems to be a holdup on marketing of GlaxoSmithKline's (GSK) new over-the-counter (OTC) weight-loss drug, Alli. In an 11 to 3 vote, an FDA advisory panel recommended approval of Alli, the OTC version of Xenical, on January 23 - over 9 months ago. GSK was thrilled and hoped to get the drug in stores before the end of this year, pending the FDA's final go-ahead. Since Alli would be the only FDA-approved weight-loss drug available without a prescription, GSK was salivating.